Every organization that touches patient data, whether a hospital, insurance company, or business associate, has a legal obligation to protect it. But knowing exactly what is protected health information (PHI) under HIPAA isn’t always straightforward. The line between general health data and legally protected information trips up even experienced compliance teams, and getting it wrong carries serious penalties.
PHI isn’t just medical records. It includes 18 specific identifiers defined by the U.S. Department of Health and Human Services that, when linked to health data, make that information identifiable to an individual. A diagnosis alone may not qualify. Pair it with a name, date of birth, or Social Security number, and it becomes PHI, subject to strict HIPAA rules on how it’s stored, shared, and secured.
For organizations managing HIPAA compliance training through platforms like Axis LMS from Atrixware, understanding PHI at this level of detail matters. Your workforce needs more than a surface-level overview; they need to recognize PHI when they encounter it and know how to handle it correctly. This guide breaks down the full definition of PHI, walks through all 18 identifiers, and provides practical examples so you can build that understanding from the ground up.
Why PHI matters for organizations
Understanding what is protected health information (PHI) isn’t just a legal formality. Organizations that handle health data face real consequences when they mismanage it, from multi-million dollar fines to criminal charges. HIPAA enforcement has grown steadily more aggressive, and the Office for Civil Rights (OCR) at HHS investigates thousands of complaints each year. If your organization touches patient or member data in any capacity, PHI compliance is a core operational responsibility, not a box to check during annual training.
The financial cost of a PHI breach
HIPAA violations carry tiered civil penalties that scale with the level of negligence involved. Unknowing violations can cost $100 to $50,000 per incident. Willful neglect that goes uncorrected starts at $50,000 per violation and can reach $1.9 million for a single violation category within a calendar year. A breach involving tens of thousands of patient records can push total penalties into the tens of millions before litigation costs even enter the picture.
Beyond civil penalties, criminal violations of HIPAA can result in prison time. Individuals who knowingly obtain or disclose PHI without authorization face up to 10 years in federal prison when the offense involves intent to sell or exploit the information for personal gain. That exposure extends to individual employees, not just executives, which means every person in your organization who handles health data carries personal liability.
When penalties can reach seven figures and carry criminal risk, PHI compliance stops being just a legal concern and becomes a business survival issue.
Reputational damage compounds the financial hit
Fines are painful, but the reputational fallout from a PHI breach often does longer-lasting damage. Patients and members lose trust quickly when their health information is exposed. IBM’s annual Cost of a Data Breach report has consistently shown that healthcare has the highest average breach cost of any industry, largely because of how difficult trust is to rebuild after an incident.
Your business partners, insurers, and vendors also factor breach history into their decisions. Many contracts now include HIPAA compliance requirements, and a documented violation can disqualify your organization from partnerships or trigger indemnification clauses. The downstream cost of lost business rarely shows up in headlines about a fine, but it consistently adds to the total impact.
PHI compliance shapes how your workforce behaves
Most PHI breaches don’t originate from sophisticated cyberattacks. They come from employee mistakes: sending an email to the wrong recipient, leaving a printed record unattended, or accessing a patient file out of curiosity rather than necessity. This is where compliance training becomes a direct line of defense rather than an administrative exercise.
Your workforce needs to understand exactly what qualifies as PHI and why it receives special legal protection. When employees can identify protected information on sight, they make better decisions in the moment, whether they’re sending a file, fielding a phone call, or coordinating with a third-party vendor. Organizations that invest in structured, role-specific compliance training consistently show lower rates of reported incidents compared to those relying solely on annual policy acknowledgments.
HIPAA definition of PHI in plain English
The Health Insurance Portability and Accountability Act (HIPAA), passed in 1996, established a specific legal definition for protected health information (PHI) that goes beyond a simple description of medical records. Understanding what is protected health information PHI at the statutory level gives you a clearer framework for identifying it in practice, rather than relying on guesswork about what qualifies.
What the statute actually says
Under HIPAA, PHI is any individually identifiable health information that a covered entity or its business associates create, receive, maintain, or transmit. The U.S. Department of Health and Human Services defines it as information relating to an individual’s past, present, or future physical or mental health condition, the provision of healthcare to that individual, or the past, present, or future payment for healthcare services.
The phrase "individually identifiable" is the pivot point in this definition. Raw health data, a general list of diagnoses or a set of lab results, only becomes PHI when it can be linked back to a specific person. That link can come from an obvious identifier like a name or Social Security number, or from a combination of data points that together make the individual recognizable.
PHI isn’t defined by how sensitive the health information feels. It’s defined by whether the data can identify a specific person.
The three-part test for PHI
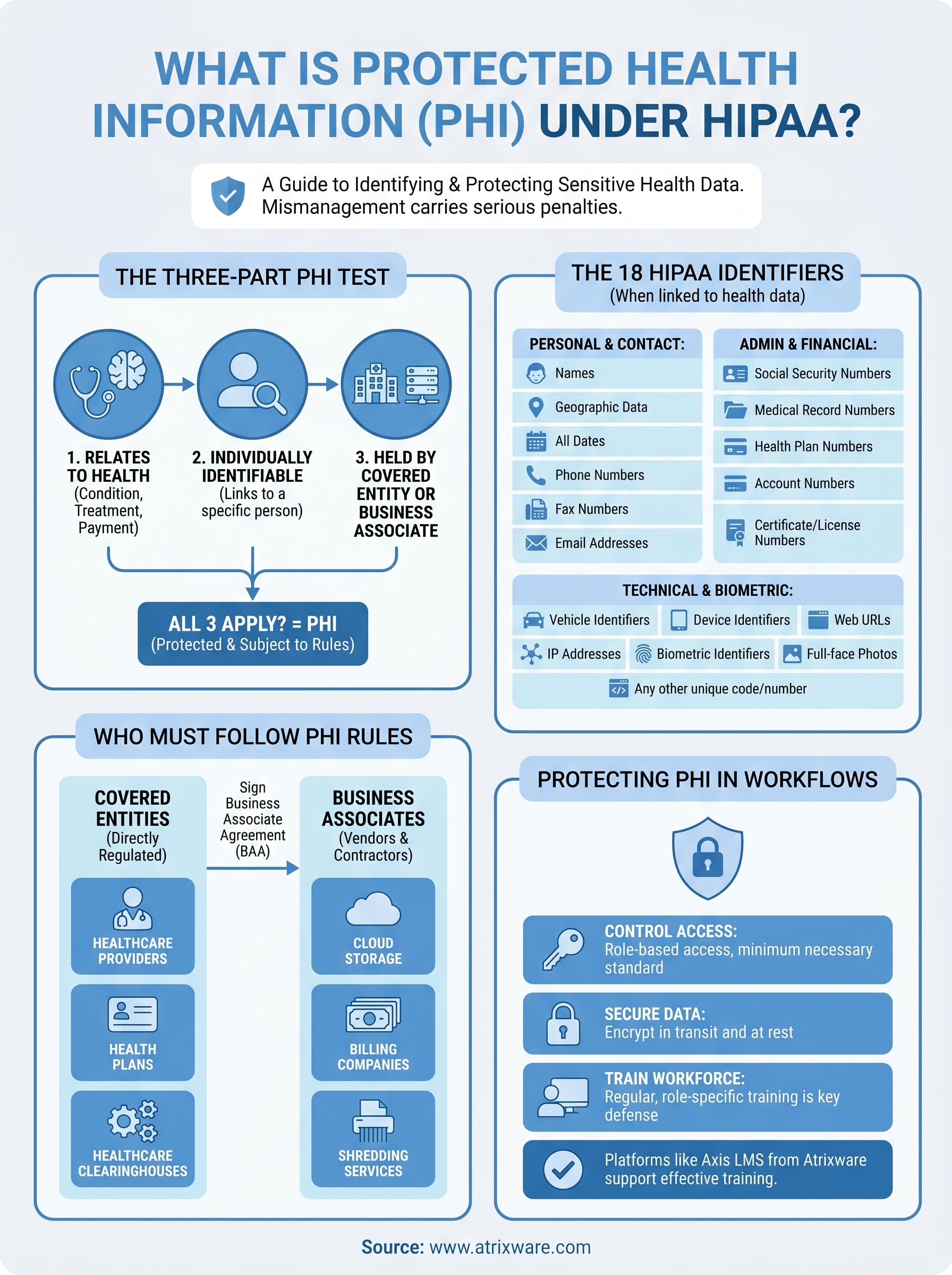
You can use a practical three-part test to determine whether information qualifies as PHI. All three conditions need to be true at the same time:
- The information relates to health: It concerns a person’s physical or mental health condition, the healthcare they received, or the payment made for that care.
- The information identifies or could identify an individual: It includes, or can be combined with, data that ties back to a specific person.
- A covered entity or business associate holds it: The information was created, received, stored, or transmitted by an organization that falls under HIPAA’s jurisdiction.
When all three conditions apply, you are looking at PHI subject to HIPAA’s full protection requirements. If any one of them is absent, the information may not qualify, though it could still fall under other state or federal privacy laws depending on your organization’s location and industry.
This framework gives your compliance training a concrete starting point. Rather than asking whether health data seems sensitive enough to protect, you ask whether it meets each condition in the test.
Who must follow PHI rules
HIPAA doesn’t apply to every organization that touches health-related data. It applies to specific categories of organizations defined in the law, and where your organization fits determines exactly what obligations you carry. Understanding this scope is the first step before you can build any meaningful compliance program around what is protected health information PHI.
Covered entities
The term covered entity refers to the three categories of organizations that HIPAA directly regulates:

- Healthcare providers: Doctors, hospitals, clinics, pharmacies, dentists, psychologists, and any provider that transmits health information electronically in connection with covered transactions.
- Health plans: Insurance companies, HMOs, Medicare, Medicaid, and employer-sponsored health plans that pay for healthcare services.
- Healthcare clearinghouses: Organizations that process nonstandard health information into a standard electronic format, acting as intermediaries between providers and payers.
If your organization falls into any one of these three categories, HIPAA’s Privacy Rule and Security Rule apply directly, and every employee who touches PHI operates under those rules regardless of their specific role.
Covered entity status isn’t optional. If your organization fits the definition, HIPAA compliance is a legal requirement, not a business decision.
Business associates
HIPAA extends its reach beyond covered entities through the business associate framework. A business associate is any vendor, contractor, or third-party service provider that creates, receives, maintains, or transmits PHI on behalf of a covered entity. This category is intentionally broad.
Examples include billing companies, cloud storage providers, EHR software vendors, legal firms that handle patient data, and even shredding companies that destroy physical medical records. If your work involves access to PHI belonging to a covered entity’s patients or members, you are a business associate and must sign a Business Associate Agreement (BAA) that legally commits you to protecting that information under HIPAA’s standards.
Subcontractors and downstream obligations
The obligation doesn’t stop at the business associate level. Subcontractors who receive PHI from a business associate carry the same HIPAA responsibilities as the business associate itself. This downstream accountability means that every link in the chain, from the covered entity to the vendor to the vendor’s subcontractor, must meet the same standard of protection for that information.
Your organization needs to actively track these relationships and confirm that BAAs flow through the entire chain. A gap anywhere in that chain, such as a subcontractor who handles data without a signed agreement, creates direct liability for the business associate above them.
What makes information identifiable
The concept of identifiability is central to understanding what is protected health information PHI. Health data doesn’t become PHI simply because it mentions a condition or treatment. It becomes PHI when it can be traced back to a specific individual, either through one obvious data point or through a combination of details that narrows the pool to a single person.
Direct identifiers
Explicit personal details represent the most straightforward path to identifiability. A patient’s full name attached to a diagnostic report connects that health record to one person immediately. Similarly, a Social Security number, phone number, or email address on a health insurance claim makes the record directly traceable with no additional data required to confirm who it belongs to. These direct identifiers work alone; they don’t need supporting details to establish identity.
When any direct identifier appears alongside health information, the combined record meets the HIPAA definition of PHI and triggers the full set of privacy and security obligations your organization must follow.
Indirect identifiers and data combinations
Indirect identifiers are harder to spot and more frequently misunderstood. A single data point like a zip code or date of birth may not identify anyone on its own. But combine that zip code with a birth date and a specific diagnosis, and the overlap of those three values can point to one individual in a small geographic area.
A combination of seemingly harmless data points can make health information just as identifiable as a name or Social Security number attached to a medical record.
Research through the National Institutes of Health has demonstrated that 87% of the U.S. population can be uniquely identified using only zip code, birth date, and gender. This finding explains why HIPAA treats combinations of indirect identifiers with the same legal weight as direct ones.
The standard for de-identification
HIPAA provides two accepted methods for removing identifiability from health data. The first is the Safe Harbor method, which requires stripping all 18 specific identifiers from a dataset. The second is the Expert Determination method, where a qualified statistician certifies that the risk of re-identification is sufficiently small for the data to be released or used without HIPAA restrictions.
Both methods carry specific requirements your organization must satisfy completely:
- Safe Harbor: Remove all 18 identifiers and verify no residual re-identification risk remains
- Expert Determination: A qualified statistician formally certifies the remaining risk is very small
Partial removal of identifiers does not satisfy either standard and leaves your organization exposed to the same HIPAA liability as fully unmodified PHI.
The 18 HIPAA identifiers
Knowing what is protected health information PHI in a technical sense matters, but your team also needs to recognize the specific data points that trigger HIPAA’s protections. The U.S. Department of Health and Human Services identifies 18 categories of information that, when combined with health data, make a record individually identifiable and therefore subject to PHI rules. Learning each one prevents the "I didn’t realize that counted" mistakes that create liability.
Personal, contact, and geographic identifiers
This first group covers the most recognizable ways a health record can point back to a specific person.
| Identifier | What it includes |
|---|---|
| Names | Full name, last name with first initial, any combination that identifies the person |
| Geographic data | Street address, city, county, zip code, or any subdivision smaller than a state |
| Dates | Birth dates, admission dates, discharge dates, death dates, and any date (other than year) directly tied to an individual |
| Phone numbers | All telephone numbers, including mobile |
| Fax numbers | Any fax contact associated with an individual |
| Email addresses | Personal or work email linked to a patient or member |
Geographic data carries more weight than most people expect. A five-digit zip code combined with a birth year and a diagnosis can identify a single individual in a small region.
Administrative and financial identifiers
These identifiers appear in billing, insurance, and administrative workflows, which makes them easy to overlook during routine processing. Your staff handling claims, credentialing, or account management encounters these regularly.
- Social Security numbers
- Medical record numbers
- Health plan beneficiary numbers
- Account numbers
- Certificate and license numbers
Each item on this list links health data to a specific individual through an administrative system. Even a partial account number that uniquely points to one person qualifies under HIPAA’s standard.
Technical and biometric identifiers
This final group covers the data types that have grown in relevance as healthcare systems become more digital and organizations collect richer data about individuals.
- Vehicle identifiers and serial numbers, including license plate numbers
- Device identifiers and serial numbers
- Web URLs associated with an individual
- IP addresses
- Biometric identifiers, including fingerprints and voice prints
- Full-face photographs and comparable images
- Any other unique identifying number, code, or characteristic
IP addresses and device identifiers belong here because healthcare applications increasingly log user activity at a technical level. If that log data touches health information, even passively, your organization must treat it as PHI and apply the same protections you would to a paper medical record.
Common PHI examples and tricky cases
Understanding what is protected health information PHI becomes much more practical when you can point to real examples from your own workflows. Some cases are obvious, but others catch compliance teams off guard because the health connection isn’t visible on the surface. Both types belong in your training program.
Straightforward PHI your team sees daily
Most employees encounter clear-cut PHI regularly without pausing to label it. A patient’s intake form that includes a name, date of birth, and diagnosis is PHI by definition. So is a billing statement that links a person by name to a specific procedure code.
Other common examples your staff should recognize immediately:
- Prescription labels displaying a patient’s name and medication
- Lab result emails addressed to a specific individual
- Insurance claim forms connecting a member ID to a treatment date
- Discharge summaries sent from a hospital to a primary care physician
Your team’s main responsibility with these records is applying access controls and the minimum necessary rule, which limits PHI exposure to only what each role requires to do its job.
Tricky cases that create unintentional exposure
Some PHI scenarios don’t resemble medical records at first glance. A photograph taken in a clinical setting qualifies as PHI when it appears in a patient’s file or connects to their care in any way. A phone log showing that a specific person called a mental health provider on a specific date can cross into PHI territory depending on the context in which that log is stored.
Any combination of an identifiable individual and a connection to their health, treatment, or payment for care is enough to produce PHI, even without a formal medical record.
Emails between a patient and a provider discussing symptoms or scheduling are PHI even when the tone is casual. Wellness program data that captures employee health screening results becomes PHI when it flows through a covered entity or business associate rather than staying isolated within the employer’s separate HR system.
When standard business data becomes PHI
Technical data like IP addresses and device identifiers enters PHI territory when your system logs tie that information to a patient’s portal activity or health record. A spreadsheet tracking which employees completed health screenings and what those results showed qualifies as PHI if your organization sponsors a group health plan subject to HIPAA. The data type itself doesn’t determine protection status; the connection to an identifiable individual’s health does.
What is not PHI and when HIPAA does not apply
Knowing what is protected health information PHI helps you stay compliant, but knowing what falls outside that definition is equally important. Not all health-related data triggers HIPAA, and misclassifying non-PHI as protected can create unnecessary operational friction, while misclassifying PHI as unprotected creates legal exposure. Getting the boundary right protects your organization on both sides.
De-identified and anonymized data
Once your organization removes all 18 HIPAA identifiers from a health record and verifies that the remaining data carries no re-identification risk, the resulting dataset is no longer PHI. De-identified data falls outside HIPAA’s Privacy Rule, which means your organization can use or share it for research, analytics, or product development without authorization requirements.
De-identification only works when it’s complete. Removing 17 of the 18 identifiers still leaves you with PHI and the full weight of HIPAA’s protections attached.
The two accepted paths to de-identification carry specific requirements your compliance team must meet:
- Safe Harbor method: Strip all 18 identifiers and verify that no residual re-identification risk remains in the dataset.
- Expert Determination method: Engage a qualified statistician who formally certifies that re-identification risk is very small and documents that finding in writing.
Data that HIPAA does not reach
Several categories of health-related information exist entirely outside HIPAA’s scope because neither a covered entity nor a business associate holds them. Employment records your organization maintains separately from your group health plan do not qualify as PHI, even when those records mention a medical condition. A manager’s note about an employee’s sick leave falls into this category when it stays within HR and never flows through a covered health plan.
Consumer wellness apps, fitness trackers, and personal health platforms your employees use independently also sit outside HIPAA. Apple Health, a running app, or a dietary tracking tool collects health data, but those companies don’t operate as covered entities or business associates, so HIPAA simply doesn’t govern them.
Education records protected under the Family Educational Rights and Privacy Act (FERPA) represent another area where HIPAA does not apply, even when those records contain health information about students. Schools and universities operating under FERPA follow a separate federal framework, and the two laws don’t overlap in standard situations.
Life insurance carriers, workers’ compensation programs, and most employer wellness programs that sit outside a group health plan also fall beyond HIPAA’s jurisdiction, though state laws may impose their own privacy requirements depending on where your organization operates.
How PHI can be used and disclosed
Understanding what is protected health information PHI also means understanding when your organization can legally use or share it and when it cannot. HIPAA doesn’t prevent all movement of protected health information; it sets specific conditions under which that movement is permitted. Knowing these conditions keeps your workflows functional without creating unnecessary compliance risk.
Permitted uses without patient authorization
HIPAA’s Privacy Rule allows covered entities and business associates to use and disclose PHI for certain purposes without obtaining a patient’s written authorization. These permitted uses exist because health operations require information flow to function. The most common ones your organization will encounter fall into three categories: treatment, payment, and healthcare operations.
- Treatment: Providers share PHI with other clinicians involved in a patient’s care, such as sending lab results to a referring physician or transferring records during a hospital admission.
- Payment: Your organization can use PHI to process claims, determine coverage eligibility, and coordinate benefits with insurers without obtaining separate authorization.
- Healthcare operations: Quality assessment, staff training, auditing, and compliance activities that keep your organization running qualify as permitted uses under this category.
Beyond these three, HIPAA also permits disclosure for public health activities, abuse reporting, law enforcement requests under specific conditions, and certain research purposes when proper oversight mechanisms are in place, such as an Institutional Review Board approval.
Even when a disclosure is permitted, your organization must apply the minimum necessary rule, sharing only the PHI that the specific purpose actually requires.
When authorization is required
For uses that fall outside the permitted categories, your organization needs a valid written authorization from the individual before accessing or sharing their PHI. This requirement applies most commonly to marketing activities, the sale of PHI to third parties, and sharing psychotherapy notes with anyone other than the treating provider.
A valid HIPAA authorization must meet specific requirements. It needs to identify the information being used, name the person or organization receiving it, explain the purpose, state an expiration date or event, and include the individual’s signature. Missing any element makes the authorization invalid, and using PHI based on a defective authorization carries the same liability as using it without any authorization at all. Your compliance training should walk staff through how to verify that an authorization form is complete before acting on it.
How to protect PHI in everyday workflows
Protecting what is protected health information PHI in day-to-day operations requires more than policies sitting in a shared drive. Your team needs concrete habits and technical controls built into the workflows they use every hour. The gap between having a compliance policy and actually protecting PHI consistently lives in the details of how work gets done.
Control access and apply the minimum necessary standard
Your first line of defense is limiting who can see PHI in the first place. Role-based access controls ensure that each employee can view only the information their job function requires, nothing more. An accounts receivable specialist has no legitimate need to read clinical notes, and a front desk coordinator shouldn’t have access to billing records outside their direct responsibilities.
Audit logs support this control by giving your organization a record of who accessed PHI and when. Reviewing those logs regularly lets you catch inappropriate access before it escalates into a reportable breach. Set up alerts for unusual activity patterns, such as bulk record downloads or access attempts outside normal working hours, so your team responds quickly rather than discovering an issue weeks later.
Secure PHI in transit and at rest
PHI moves constantly through your workflows: emails, file transfers, cloud storage, and printed documents all carry risk if left unprotected. Encrypting PHI at rest and in transit is the baseline technical safeguard your organization needs to meet HIPAA’s Security Rule requirements. Any email containing PHI should travel through an encrypted channel, not a standard unprotected inbox.
Encryption doesn’t eliminate the need for access controls. A well-encrypted file sent to the wrong recipient is still a breach.
Physical PHI demands the same attention. Printed records and fax transmissions must be handled with the same care as digital files. Workstations displaying patient data should lock automatically after a short idle period, and printed documents should move directly to a secure location rather than sitting on an unattended desk or shared printer tray.
Train your workforce to recognize risks before they become incidents
Technology controls reduce risk, but employee behavior is where most PHI incidents originate. Your staff needs regular, role-specific training that goes beyond an annual policy acknowledgment. When your team understands exactly which data qualifies as PHI and why it’s protected, they make better decisions in the moment rather than discovering the problem after an email has already been sent.
Scenario-based training that mirrors real situations your employees face builds the recognition skills that protect your organization in practice. Platforms like Axis LMS allow you to deliver that training efficiently, track completion, and document compliance across your entire workforce.
A quick recap
What is protected health information PHI comes down to one core principle: any health data that can be traced back to a specific individual, held by a covered entity or business associate, falls under HIPAA’s full protection requirements. The 18 identifiers define the boundaries of identifiability, and those boundaries apply whether the data lives in a paper file, an email inbox, or a cloud-based system. Permitted disclosures exist, but even those carry the minimum necessary standard. Most breaches trace back to employee decisions made in the moment, which is why structured, role-specific training matters more than annual policy reviews.
Your workforce needs to recognize PHI on sight and know exactly how to handle it. Building that recognition takes consistent, well-structured training delivered to every role that touches health data. If you’re ready to see how a purpose-built platform can support that effort, start your Axis LMS admin demo and explore what compliance training at scale looks like in practice.